A main goal following Total Knee Arthroplasty (TKA) is, in addition to pain relief, restoration of function. A continuous passive motion (CPM) machine is frequently used to help achieve this goal. However the efficacy of the CPM machine has not been consistently supported in the research. Brousseau et al in a metaanalysis of the efficacy of passive motion following TKA showed that CPM combined with physical therapy may offer beneficial results for patients but these benefits must be weighed against the inconvenience and expense of the CPM. 2
The CPM machine is heavy and cumbersome. It requires assistance from caregivers for proper use and positioning in the machine and is a risk to caregivers given the size and weight of the machine. CPM machines are also a challenge to patients that are short or obese as the machines are not custom fit to the patient and only come in standard sizes. Improper positioning can cause stress to the knee and cause the patient to be uncomfortable during use. It also must be used mainly in bed secondary to the size of the machine and use in a chair or couch could be unsafe.
A more portable alternative to the CPM machine may produce better compliance, edema control and achieve the desired post operative range of motion seen with the CPM. It is thought that edema control is one of the keys to successfully regaining knee function following TKA. Our hypothesis is that coupling edema control, through appropriate positioning and elevation, will a standard exercise protocol with yield desirable ROM that is equal to the results seen with CPM coupled with a standard exercise protocol. One hypothesis is achieving and maintaining full extension with positioning in the acute postoperative phase will lead to better outcomes for post operative extension. Focusing on edema control will lead to optimal outcomes for post operative flexion and leg control. A dense foam pillow (LRU 2031) (Fig. 2) was specially designed to achieve these goals. It maintains the knee in an extended position while elevating the lower extremity to help with edema control. We believe that patients will achieve at least the same results of active assistive ROM and visual analog pain scores using the LRU pillow with a standard physical therapy protocol in a more cost effective way than those using the CPM with a standard physical therapy protocol.
Materials and Methods:
This prospective randomized control trial was approved by the institutional review
board at our hospital. Patients receiving total knee arthroplasties from the senior investigators office were randomized (by SPSS 11.0 (SPSS Inc., Chicago, IL)) to either receive a CPM machine post operatively or LRU pillow. Twenty patients were enrolled, ten in each group. The CPM machine and LRU pillow were used 2 hours on and 2 hours off from 8am to 10 pm. It was then used continually from 10pm to 8am.
Five days prior to surgery baseline pain scores, using the analog pain score, and active assistive ROM of the operative knee were obtained. All patients then underwent TKA performed by the senior investigator. Patients then were randomized and received either a CPM machine or LRU pillow in the PACU following surgery. The end of hospital stay was defined as completion of physical therapy on post operative day 2. At this point post operative active assistive knee range of motion and pain scores were recorded. After discharge the patient was instructed to continue using either CPM or LRU for 18 hours a day until their follow up visit on post operative day 16. At this point all patients were instructed to not use their CPM/LRU from this point on. Final active assistive knee ROM and pain scores were collected 2 months post operatively.
Active assistive range of motion of the surgical knee was measured with the use of a long arm goniometer, aligned against anatomical landmarks, by a physical therapist or physical therapist assistant. Active assistive ROM was defined as a exercise in which an external force assists specific muscles and the knee joint to move through the available excursion. Measurements were taken with the patient lying supine. Active assistive ROM was recorded 5 days preoperatively, 2 days post operatively, 16 days post operatively and 2 months post operatively.
Each patient was treated with the same peri-‐operative pain regimen. This consisted of 15mg Toradol IV pre-‐operatively and every 6 hours post operatively during their hospitalization. 150mg of Lyrica PO was given pre-‐operatively and 75mg BID was given post operatively during their hospitalization. Post operatively each patient also received scheduled 1000mg of Tylenol every 6 hours and 5-‐10mg of Oxycodone every 4 hours. At discharge every patient was given Tylenol 100mg every 6 hours, Celebrex 200mg BID, Oxycodone 5-‐10mg every 4 hours PRN and Lyrica 75mg BID. This regimen was continued until post operative day 16 at which time patients were instructed to use these pain medications as needed.
Differences between the study groups with respect to age were analyzed using the T test and the Mann Whitney Test. Differences with respect to sex were analyzed using Fisher’s Exact Test. The differences between pain scores and active assistive ROM at 5 days pre-‐operatively, 2 days post operatively, 16 days post operatively and 2 months post operatively were also compared between our two groups and analyzed using the T Test and the Mann Whitney Test. A p value of < 0.05 was considered significant.
Results:
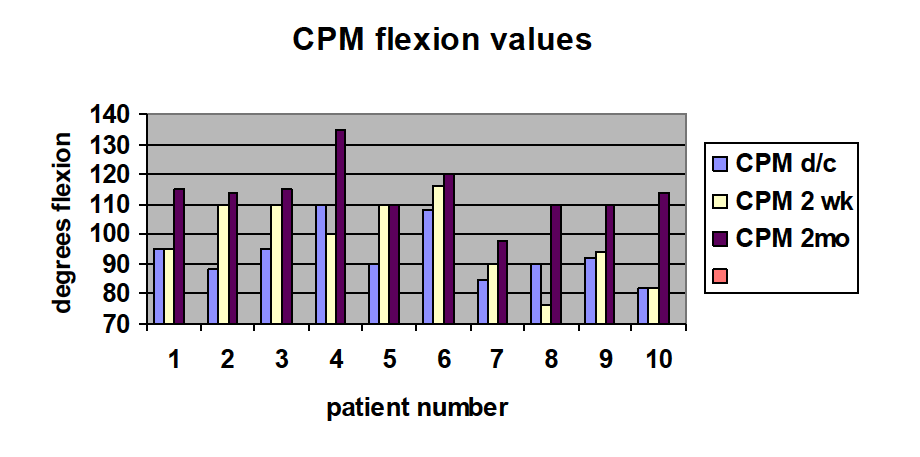
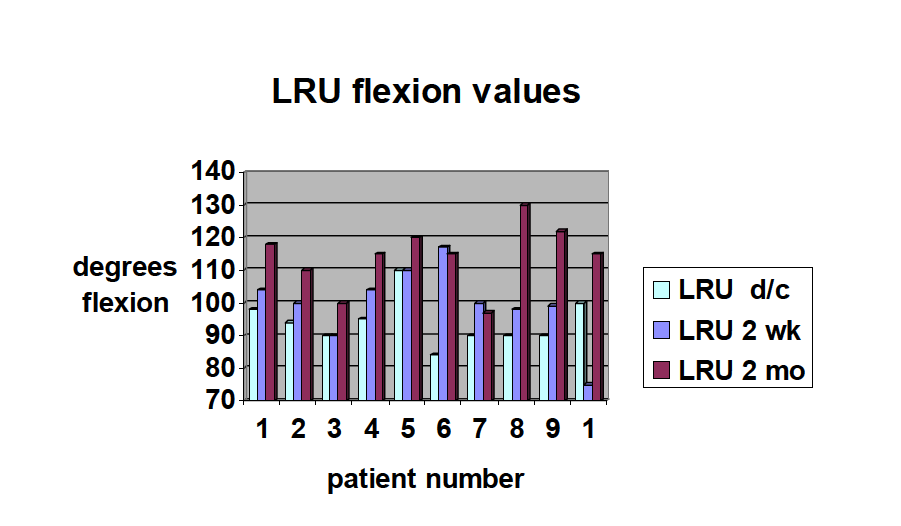
Ten patients were randomized to receive the CPM machine post operatively and ten patients were randomized to receive the LRU pillow post operatively. The groups were analyzed with regards to age and sex. There were 3 males and 7 females in each group. The average age was not statistically significant (p= 0.239, 0.686) and for the CPM group was 66 (+/-‐ 9) and for the LRU group was 62.8 (+/-‐7). Tables 1 and 2 summarizes the flexion numbers for CPM and LRU groups, respectively. There was no difference in the ROM in extension or flexion at any time point. The average flexion at discharge was 93 and 94, at 2 weeks was 98 and 100, and at 2 months was 114 and 114 degrees respectively between CPM and LRU groups. There was no difference in the pain scale numbers at any point between groups.
Table 1:
Discussion:
The use of CPM machine post operatively in patients who have undergone TKA is a standard practice along with a physical therapy program. Our study hypothesized that the benefits seen with a CPM machine can be achieved with a lower cost and a more convenient LRU pillow. We believe that the pillow contributes to similar post operative ROM and pain due to positioning of the leg in extension and elevation. The LRU pillow is also cost effective when compared with the CPM machine. (See attachment). At our institution the cost of the LRU pillow is $80.00 while the cost of the CPM is $90 -‐ $240 ($30-‐60/day for 2 to 3 day hospital stay). Extended usage to 2 weeks would increase the range to $450-‐900. The patient then has no access beyond 2 weeks.
Numerous studies have shown mixed results with regards to post operative ROM, pain control and length of hospital stay with the use of CPM machine. Brousseau et all showed that the CPM machine was beneficial but must be weighed against the inconvenience and cost associated with the CPM. The LRU pillow shows equivalent results as the CPM without the inconvenience or cost.
Our study has shown that patients who used the LRU pillow had as good of results as those using the CPM machine post operatively. There were several limitations to this study.
Firstly, our sample size was small. Secondly, although all patients stated compliance to the study protocol we had no way to ensure this.
With regards to each group, they did not differ significantly when comparing age and sex but we did not analyze to see if they differed in weight, height , BMI or co-‐morbidities. Each of these factors could have contributed to the post operative outcome. When evaluating each patient pre and post operatively several physical therapists were involved in each patients care. This could lead to variable active assistive ROM measurements at each follow up.
In conclusions, our study was able to show a cost effective and convenient alternative to the CPM machine that achieves equivalent results when paired with a standard physical therapy program and pain regimen. Further studies will need to be conducted with larger patient samples to validate this study but it does show a promising alternative to the CPM machine that can contribute to decreased hospital costs and improved patient safety.
Bibliography:
- Beaupre LA, Davies DM, Jones CA, Cinats JG. Exercise combined with continuous passive motion or slider board therapy compared with exercise only: a randomized controlled trial of patients following total knee arthroplasty. Phys Ther. 2001 Apr.81(4):1029-‐37.
- Brosseau L, Milne S, Wells G, Tugwell P, Robinson V, Casimiro L, Pelland L, Noel MJ, Davis J, Drouin H. Efficacy of continuous passive motion following total knee arthroplasty: a metaanalysis. J Rheumatol. 2004 Nov;31(11):2251-‐64.
- BrunnOlsen V, Heiberg KE, Mengshoel AM. Continuous passive motion as an adjunct to active exercises in early rehabilitation following total knee arthroplasty-‐a randomized controlled trial. Disabil Rehabil. 2009;31(4):277-‐83.
- Chen B, Zimmerman JR, Soulen L, DeLisa JA. Continuous passive motion after total knee arthroplasty: a prospective study. Am J Phys Med Rehabil. 200 Sep-‐Oct;79(5):421-‐6.
- Denis M, Moffet H, Caron F, Oullet D, Paquet J, Nolet L. Effectiveness of continuous passive motion and conventional physical therapy after total knee arthroplasty: a randomized clinical trial. Phys Ther. 2006 Feb;86(2):174-‐85.
- Harvey LA, Brosseau L, Herbert RD. Continuous passive motion following total knee arthroplastyin people with arthritis. Cochrane Database Syst Rev. 2010 Mar 17;3 CD004260.
- Lenssen TA, van Steyn MJ, Crijns YH, Waltje EM, Roox GM, Geesink RJ, van den Brandt PA, De BieRA. Effectiveness of prolonged use of continuous passive motion (CPM), as an adjunct to physiotherapy, after total knee arthroplasty. BMC Musculoskelet Disord. 2008 Apr 29;9:60.
- Postel JM, Thoumie P, Missaoui B, Biau D, Ribinik P, Revel M, Rannou F. Continuous passive motion compared with intermittent mobilization after total knee arthroplasty. Elaboration of French clinical practice guidelines. Ann Redaapt Med Phys. 2007 May;50(4):244-‐57. Epub 2007 Mar 19.
- Shi MG, Lu HS, Guan ZP. (influence of preoperative range of motion on the early clinical outcome of total knee arthroplasty). Zhonghua Wai Ke Za Shi. 2006 Aug 15;44(16):1101-‐5.